
Dr. Yong Cui pioneered no-visible-scar, trans-axillary cardiac surgery in China — and originated MESM, Minimally Invasive Electro-Septal Myectomy.
Director, Department of Cardiovascular Surgery — Heart Center, Zhejiang Provincial People's Hospital (Affiliated People's Hospital, Hangzhou Medical College).
Every heart operation has the same purpose — to make the heart whole again. When the anatomy allows, that same repair can be done through a single hidden incision beneath the arm: the sternum is spared, there is no visible scar, and recovery often begins sooner.
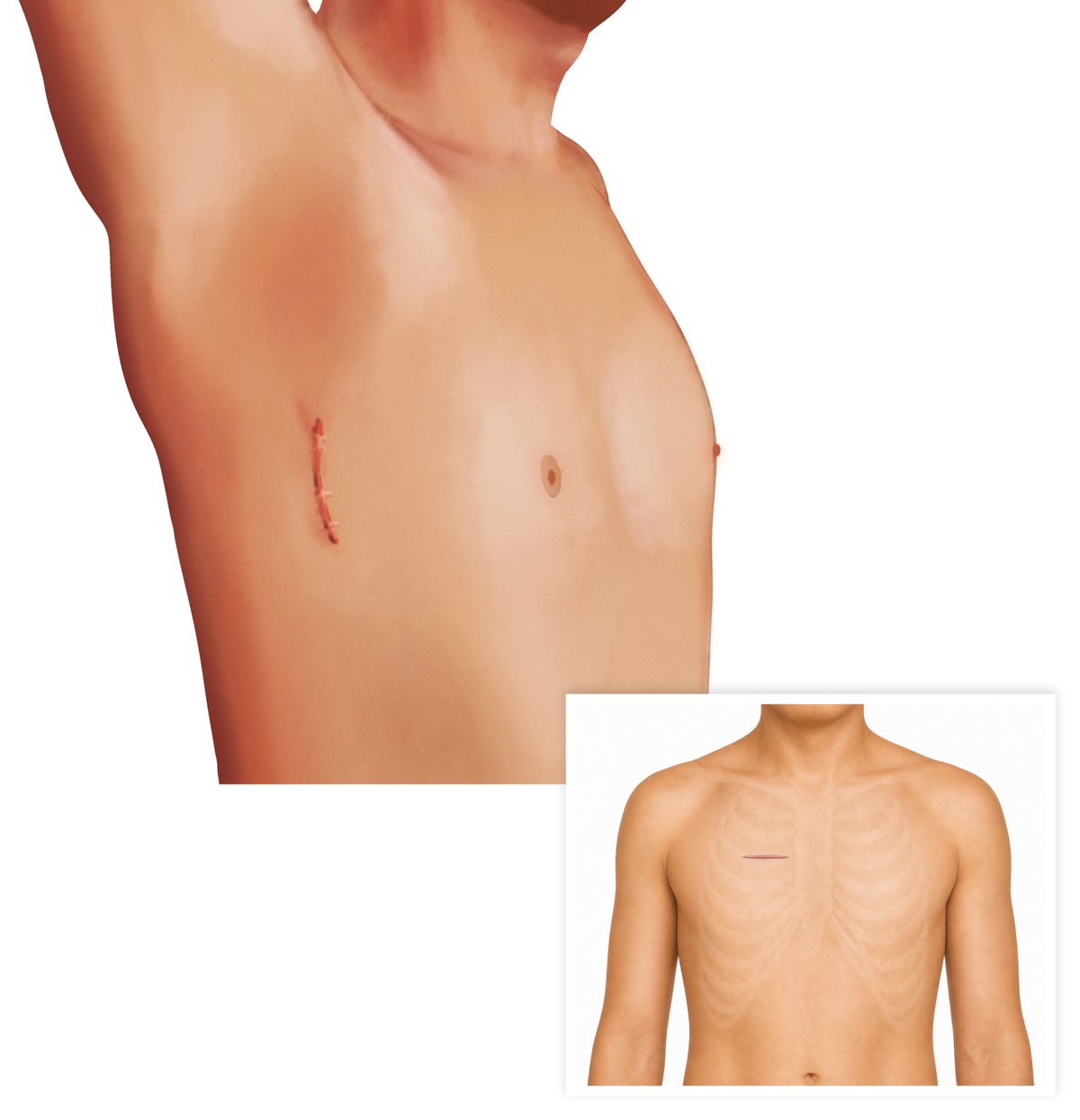
The great majority of operations are done through a single 5 cm trans-axillary incision between the anterior and mid-axillary line — with the arm at rest, nothing shows on the front of the chest. It is the only incision: no separate camera ports, no drainage ports, no left-atrial retractor ports. For aortic-root and selected valve work, a short anterior right-thoracotomy incision beside the sternum is used instead. In every case the sternum stays intact, so the risk of sternal wound and mediastinal infection is eliminated entirely.
The great majority of operations are performed through the trans-axillary no-scar approach. Aortic root reconstruction and aortic valve repair — which cannot be reached from the axilla — are performed through a right parasternal minimally invasive incision. In both, the sternum is never divided.
Almost the entire spectrum of cardiac surgery, performed through a single 5 cm incision hidden beneath the arm — no sternotomy, no visible scar.
Aortic root reconstruction and aortic valve repair cannot be reached from beneath the arm. These operations are performed through a small right anterolateral, parasternal minimally invasive incision — sparing the sternum while giving the direct, front-on exposure the aortic root demands. It is the most technically advanced part of the practice, and the area where repair — preserving the patient's own valve — matters most.
For advanced heart failure, a left ventricular assist device can be implanted through two small incisions — without splitting the breastbone (sternum). In 2022 Dr. Cui performed China's first reported minimally invasive, beating-heart LVAD implantation: the heart keeps beating throughout, and most patients are extubated on the first day.

The cosmetic result is what patients notice first — but it is not the point. Preserving the sternum and minimising surgical trauma means less pain, less bleeding, fewer wound complications and an earlier return to ordinary life. Minimally invasive should mean safer and faster, not merely smaller.
That principle is made concrete by an ultra-fast-track anaesthesia programme developed with the anaesthesia team: suitable patients are extubated on the operating table and out of bed early.
In obstructive cardiomyopathy, relief of obstruction is planned around the three determinants of LVOTO — septal hypertrophy, intraventricular structural abnormality, and mitral-valve geometry — rather than wall thickness alone.

Yong Cui, MD, PhD, is Director of the Department of Cardiovascular Surgery at Zhejiang Provincial People's Hospital. A Clinical Fellow at the University of Alberta (2010–2013), he returned to build one of China's most comprehensive no-scar minimally invasive cardiac programmes — and to develop MESM, his original technique for obstructive cardiomyopathy.
Director of the Department of Cardiovascular Surgery, Zhejiang Provincial People's Hospital. Clinical Fellow in cardiac surgery, University of Alberta (Mazankowski Heart Institute), Canada, 2010–2013.
An active SCI record in minimally invasive technique and outflow-tract surgery — see selected publications below.
Selected from 20+ peer-reviewed publications. Full bibliography available on request.
Operative footage and conference lectures. Surgical videos will be embedded below; talks are available now on the channel.

Enquiries are welcome from patients considering minimally invasive cardiac surgery and from physicians seeking referral, second opinion, or technique collaboration.